
Clinical Pearls: Is it DKA or HHS?
Should be pretty straight forward, but even amongst seasoned providers this can sometimes be debatable. Especially when you don’t have all the labs back. Often we are called to admit a patient for DKA because they do not seem appropriate for a routine floor or even step-down ICU admission. The Internal Medicine/Hospitalist team may not feel comfortable taking a patient but on your evaluation they do not seem to be on the severe end of the spectrum. You aren’t alone, my friend. Let’s talk about admitting a DKA vs HHS patient and the step-wise approach I take.

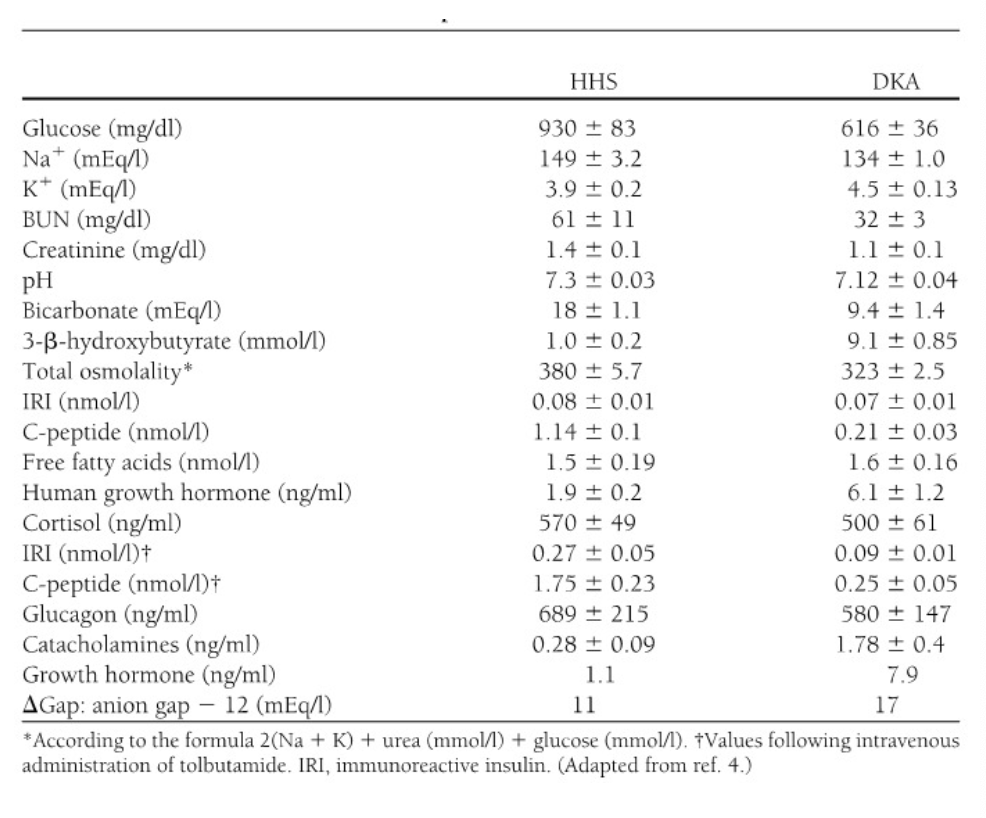
https://pubmed.ncbi.nlm.nih.gov/7808097/
Why is it confusing? Rarely in the real world practice of medicine do textbook clinical pictures arise. The norm is a combination of problems which overlap creating a diagnosis that could be attributed to multiple derangements. For example, if the diagnosis of DKA requires acidosis we must consider all the reasons one might have an elevated anion gap acidosis - how often do you find a potential DKA pt in a state of renal failure as well? Is the renal failure causing the acidosis or is DKA the culprit? Add to this the body’s natural drive to compensate creating a mixed acid base disorder. Or what about the acidotic patient who has ketones but BG is normal (is it euglycemic DKA or alcoholic or starvation ketoacidosis)? It’s enough to pull your hair out when trying to assign a diagnosis to the issue. The objective of this article is to help you make the initial differential diagnosis easier.
Before we get into the classifications, can we clear up the endless nomenclature? Not sure how we end up with so many names for the same pathophysiological state but here we are. HHNS (hyperosmolar hyperglycemic nonketotic syndrome); HHNK (Hyperosmolar hyperglycemic nonketotic coma); HHS (hyperosmolar hyperglycemic syndrome) are essentially all referring to the same state. HHNK refers to the extreme end of this involving coma. The accepted terminology at this time is HHS and this how I will refer to this state for the remainder of this text.
To further confuse things HHS can, although less commonly, occur in a type 1 diabetic and DKA can occur in a type 2 diabetic. So how do we keep things straight? Start with a basic understanding that at it’s core HHS is a state of relative insulin resistance (still just enough working insulin to prevent the body from heading into full on ketone production and acidosis) whereas DKA is an absolute insulin deficiency (no insulin available or functional enough to move glucose into the cell) resulting in acidosis. In HHS you can get by for a while while the body limps along still pushing glucose into the cell and preventing full on deranged compensation. Over time, the balance of serum glucose grows and grows. This is how you can end up with super high levels of hyperglycemia and yet not have ketonemia or ketonuria. In DKA the cells get nothing so the body compensates by breaking down fat leading to ketonemia (elevated serum beta-hydroxybuterate level). Both of these processes are complicated because our inherently wise body has developed many compensatory pathways and so this can occur on a spectrum, some of which crosses over. You can actually have both HHS and DKA simultaneously. Grr. So let’s break it down into categories.
(Key factors highlighted)
HHS
Develops slowly (days to weeks)
Absent or minimal ketosis = low or no BHB in blood or ketonuria
Absent or minimal acidosis
Won’t have as much of the acidosis clinical signs:
Like Kussmauls, confusion, abd pain, n/v, acetone breath
Serum bicarb will be near normal
AG may or may not be elevated
Glucose levels rise -> hyperosmolar blood + diuresis
High osmolality -> diuresis (lots of H20 and some electrolyte loss)
If serum osm > 320 more likelihood of altered GCS
So if your pt is in a coma and osm is <320 look for another cause
Dehydration -> impaired kidney fxn
In general will see more coma/altered GCS, severity of dehydration
DKA
Develops rapidly (hours)
Ranges in severity
Commonly precipitated by lack of insulin or infection, although there are other indications (MI, CVA, PE, pancreatitis, alcohol, drugs)
Ketones present in urine and blood (BHB will be elevated)
Acidosis is present on ABG and CMP
Will have acidosis clinical signs:
Like Kussmauls, confusion, abd pain, n/v, acetone breath
Serum bicarb will be low
AG will be high
Less severe hyperosmolality
Glucose mediated osmotic diuresis -> Dehydration
In general will see less coma/altered GCS
https://www.ncbi.nlm.nih.gov/books/NBK279052/
Common factors in both:
High BG -> Increased thirst, weight loss, increased urination, s/s of dehydration
High BG -> osmotic diuresis -> water loss + electrolyte loss (water more than electrolytes, including sodium) -> dehydration
High serum BG -> osmosis -> fluid is pulled out of cells to vasculature -> Pseudohyponatremia from dilution of sodium. Calculate a corrected Na level. If it is still low check the triglyceride level.
Insulin deficiency -> hyperkalemia (needs insulin to enter the cells)
If DKA excess H+ ion is hidden in the cell so K shifts to extracellular space which also raises this level (although the total body K may not be high).
Because of these factors if your K is low on admission you cannot start an infusion until you replace the K. Once you throw insulin into the mix your serum K will drop lower.
Treatment. Well I’m not going into extensive detail here. You will have institutional protocols that will likely drive this. The focus of management for both is volume repletion and insulin infusions. With both you should be concerned about GCS. In HHS the hyperosmolar state is the real problem with major concerns of: dehydration and AMS/coma. Your approach is a focus on fluid resuscitation and monitoring of GCS. In DKA the acidosis is the major problem and your management focuses on correcting K, starting insulin, trending the AG, and monitoring the pt for continued effective respiratory compensation of the metabolic acidosis. That’s why the DKA patient with a co-morbid condition affecting neuro status or respiratory center is the most concerning.

Click the photo to see a TT video on normal metabolic acidosis compensation.